
Order Code
2835
Preferred Specimen
Type: Serum
Volume: 2 mL
Collection Instructions:
Store refrigerated.
Collect in a Serum Separator Tube (SST).
Allow to clot upright for at least 30 minutes.
Centrifuge within 2 hours of collection.
ContainerType
Serum separator tube
Alternate Specimen Requirements
Plain Red Top Tube:
2 mL serum
Allow sample to clot upright for 60 minutes
Centrifuge and transfer serum to a plastic transport tube within 2 hours
Clearly label as: “Serum from plain red top tube”
Store refrigerated
Lithium Heparin Plasma (Green Top):
2 mL lithium heparin plasma
Centrifuge and separate plasma from cells immediately
Transfer plasma to a plastic transport tube
Clearly label as: “Lithium heparin plasma”
Store refrigerated
Note: Lithium heparin should only be used for primary testing
Minimum Volume
0.75 mL serum
Pediatric volume: 0.25 mL serum (does not allow for repeat
or additional testing).
Transport Temperature
Refrigerated
Expected Turnaround Time
1 day
Specimen Stability
8 days room temperature; 2 weeks refrigerated; 2 years frozen. Allow only one freeze/thaw cycle
Methodology
Roche COBAS Electrochemiluminescent Immunoassay (ECLIA) this method has been standardized against the 2nd irp WHO reference standard 80/558.
Overview
Thyroid Stimulating Hormone (TSH), or thyrotropin, is produced by the anterior pituitary and regulates thyroid hormone synthesis (T3, T4) through stimulation of the thyroid gland. It is regulated by thyrotropin-releasing hormone (TRH) from the hypothalamus and subject to negative feedback from circulating levels of T3 and T4.
The third-generation TSH assay used here detects down to ~0.005 mU/L and is the preferred screening test for thyroid dysfunction in stable patients.
Unlike T3/T4, TSH is not protein-bound, making it unaffected by changes in carrier protein levels due to pregnancy, steroids, liver/kidney disease.
Clinical Significance
Screen for thyroid dysfunction
Diagnose hypo-/hyperthyroidism
Monitor thyroid replacement therapy
Guide TSH suppression therapy in thyroid cancer patients
Assess patients with:
- Goiter
- Palpitations
- Unexplained weight change
- Fatigue
- Depression
Newborn screening for congenital hypothyroidism
Additional Information
Appropriate age to initiate TSH screening differs based on source. The American Thyroid Association advises every 5 years starting at age 35; the American Association of Clinical Endocrinologists advises screening women starting at age 50; and the U.S. Preventive Services Task Force (USPSTF) does not advise screening asymptomatic adults.
Patients on a steady replacement dose of T4 should have levels checked annually.
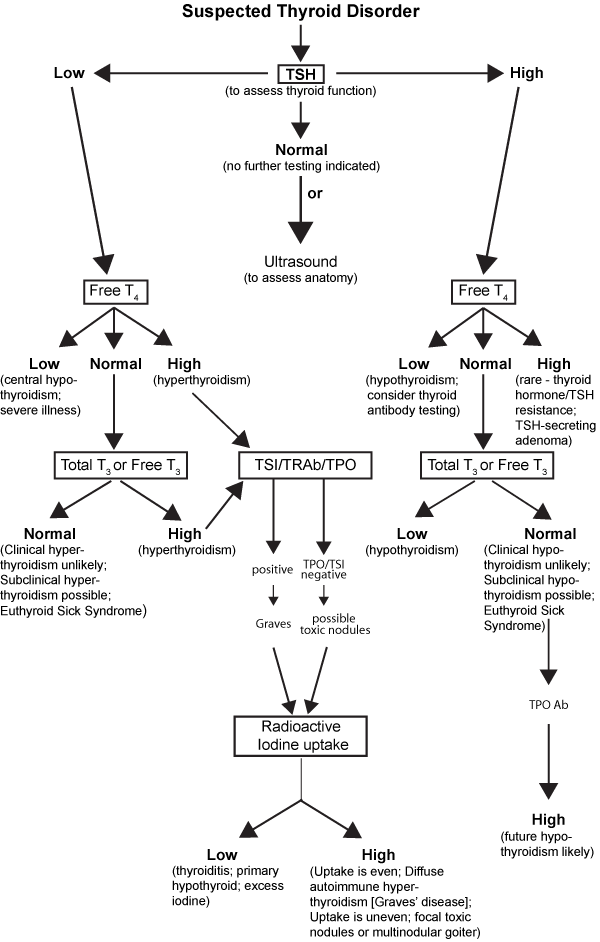
Interpretative Information
The third generation sensitive TSH (sTSH) can identify most cases of hypothyroidism and hyperthyroidism. In the setting of a healthy hypothalamic-pituitary-thyroid (HPT) axis, when peripheral T4 levels are low, the intact feedback loop results in increased pituitary TSH production. When peripheral T4 levels are high, pituitary TSH secretion is decreased. Exceptions to this generalization occur when there is damage to the hypothalamus or pituitary, alterations to normal HPT axis functioning due to medication (including recent changes in thyroxine therapy) (Guber, 2012), or nonthyroidal illness (euthyroid sick syndrome). Rarely a TSH-secreting tumor or thyroid hormone resistance can yield misleading results (Dayan, 2001).
In situations where the HPT axis is not functioning normally, or there is clinical concern of medication interference, TSH levels may be misleading and not consistent with clinical observations. In these cases, measuring the free T4 and/or free T3 levels may be helpful in clarifying the diagnosis.
Decreased TSH:
- Primary hyperthyroidism
- Subclinical hyperthyroidism
- Central hypothyroidism
- Acute nonthyroidal illness (ie, euthyroid sick syndrome)
- Drugs (eg, glucocorticoids, dopamine, amiodarone, bromocriptine)
- Over-the-counter supplements (eg, tyrosine, kelp, iodine)
- Surreptitious ingestion of thyroxine
Increased TSH:
- Primary hypothyroidism
- Subclinical hypothyroidism
- TSH-related conditions (eg, pituitary tumor or thyroid hormone resistance)
- Malabsorption of prescribed thyroxine (eg, small intestinal disease, cholestyramine)
- Drugs (eg, amiodarone, iodine, lithium, methimazole, propylthiouracil, radioiodine contrast)
False-normal TSH:
Central hypothyroidism due to pituitary or hypothalamic dysfunction
Early thyrotoxicosis
Subacute thyroiditis
Limitations
- TSH is accurate only in steady-state conditions, which are present 4-6 weeks after starting or adjusting levothyroxine dose.
- Important to remember that it takes several weeks for TSH level to accurately reflect the current thyroxine concentrations following thyroid replacement therapy, thyroid ablation, or antithyroid medication for hyperthyroidism.
- High circulating levels of biotin can interfere with thyroid function assays, most commonly causing falsely high levels of T3, free T3 and free T4 and falsely low levels of TSH, leading to an incorrect diagnosis of hyperthyroidism or conclusion that thyroid hormone dose is too high. Results inconsistent with clinical picture should be investigated (Li 2017).
References
Abalovich M, Amino N, Barbour LA, et al, “Management of Thyroid Dysfunction During Pregnancy and Postpartum: An Endocrine Society Clinical Practice Guideline,” J Clin Endocrinol Metab, 2007, 92(8 Suppl):S1-47.17948378
American Academy of Pediatrics, Rose SR; Section on Endocrinology and Committee on Genetics, American Thyroid Association, Brown RS; et al, “Update of Newborn Screening and Therapy for Congenital Hypothyroidism,” Pediatrics, 2006, 117(6):2290-303.16740880
American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, “Revised American Thyroid Association Management Guidelines for Patients With Thyroid Nodules and Differentiated Thyroid Cancer,” Thyroid, 2009, 19(11):1167-214.19860577
Baloch Z, Carayon P, Conte-Devolx B, et al, “Laboratory Medicine Practice Guidelines. Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease,” Thyroid, 2003, 13(1):3-126.12625976
Baskin HJ, Cobin RH, Duick DS, et al, “American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the Evaluation and Treatment of Hyperthyroidism and Hypothyroidism,” Endocr Pract, 2002, 8(6):457-69.15260011
Bowen R, Benavides R, Colón-Franco JM, et al. Best practices in mitigating the risk of biotin interference with laboratory testing. Clin Biochem. 2019;74:1-11.31473202
Dayan CM, “Interpretation of Thyroid Function Tests,” Lancet, 2001, 357(9256):619-24.11558500
Galarza JB. Thyroid function tests. In: Farwell A, ed. Clinical Thyroidology for the Public. Falls Church, VA: American Thyroid Association; 2018:11(12):3-4. https://www.thyroid.org/wp-content/uploads/publications/ctfp/volume11/issue12/ct_public_v1112_3_4.pdf. Accessed July 22, 2020.
Garber JR, Cobin RH, Gharib H, et al, “Clinical Practice Guidelines for Hypothyroidism in Adults: Co-Sponsored by American Association of Clinical Endocrinologists and the American Thyroid Association, Endocr Pract, 2012, 11:1-207.22967432
Gharib H, Papini E, Paschke R, et al, “American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules,” Endocr Pract, 2010, 16 Suppl 1:1-43.20497938
Guber HA and Farag AF, “Evaluation of Endocrine Function,” Henry’s Clinical Diagnosis and Management by Laboratory Methods, 22nd ed, McPherson RA and Pincus MR, eds, Philadelphia, PA: Elsevier, 2012, 365.
Katzman BM, Lueke AJ, Donato LJ, Jaffe AS, Baumann NA. Prevalence of biotin supplement usage in outpatients and plasma biotin concentrations in patients presenting to the emergency department. Clin Biochem. 2018;60:11-16.30036510
Leavelle DE, Mayo Medical Laboratories Interpretive Handbook, Rochester, MN: Mayo Medical Laboratories, 1997, 502-3.
Li D, Radulescu A, Shrestha RT, et al. Association of Biotin Ingestion With Performance of Hormone and Nonhormone Assays in Healthy Adults. JAMA. 2017;318(12):1150-1160. doi:10.1001/jama.2017.1370528973622
Luong JHT, Vashist SK. Chemistry of Biotin-Streptavidin and the Growing Concern of an Emerging Biotin Interference in Clinical Immunoassays. ACS Omega. 2019;5(1):10-18.31956746
Smallridge RC, “Disclosing Subclinical Thyroid Disease. An Approach to Mild Laboratory Abnormalities and Vague or Absent Symptoms,” Postgrad Med, 2000, 107(1):143-6, 149-52.10649671
Toft AD, “Clinical Practice. Subclinical Hyperthyroidism,” N Engl J Med, 2001, 345(7):512-6.11519506
Umpierrez GE, “Euthyroid Sick Syndrome,” South Med J, 2002, 95(5):506-13.12005007
Whitley RJ, “Thyroid Function,” Tietz Textbook of Clinical Chemistry, 3rd ed, Burtis CA and Ashwood ER, eds, Philadelphia: WB Saunders Co, 1999, 1496-529.
Diagnostic Role
- Hypothyroidism represents a deficiency in thyroxine (T4) output relative to physiologic requirements.
- Primary hypothyroidism: Failure of the thyroid itself to secrete thyroid hormone resulting in low T4 and T3 levels, with the subsequent increase in TSH release by the pituitary. The most common cause is treatment for hyperthyroidism by radioactive iodine ablation or surgery. TSH elevation precedes a measured decreased in T4 (total or free).
- Central hypothyroidism: Pituitary or hypothalamic dysfunction resulting in decreased TSH secretion (and TRH in the latter). TSH may be within or even slightly above reference range, but still too low relative to concurrently drawn low T4 levels.
- Subclinical hypothyroidism: Elevated TSH with normal levels of T4 and T3; often due to thyroiditis or inadequate treatment of hypothyroidism. Presence of thyroperoxidase (TPO) antibodies increases risk of subsequent hypothyroidism, especially if free T4 is marginally decreased.
- Hyperthyroidism represents an excess of thyroxine (T4) output relative to physiologic requirements.
- Primary hyperthyroidism: Thyroid gland overproduction of thyroxine, resulting in down-regulation of TSH levels. TSH decrease precedes a measured increase in T4 (total or free).
- Secondary hyperthyroidism: TSH levels increased due to TSH-secreting pituitary tumor (uncommon).
- Subclinical hyperthyroidism: Low TSH with normal levels of T4 and T3; typically due to excessive thyroid hormone replacement.
- Euthyroid sick syndrome: Severe nonthyroidal illness (eg, sepsis) may transiently affect thyroid hormones, binding proteins, and TSH concentrations resulting in abnormal laboratory values in a patient that does not have thyroid disease, a condition referred to as “euthyroid sick syndrome”. The TSH, T3, and T4 tend to decrease during acute illness, with return to normal or even elevated levels as the underlying condition resolves. Further complicating matters is that commonly used medications (eg, glucocorticoids, dopamine, opioids) affect TSH. Differentiation from inherent thyroid disease can be difficult biochemically. A clue to true thyroid disease would be findings of a goiter or thyroid nodule; a normal or elevated serum cortisol level favors euthyroid sick syndrome, whereas decreased serum cortisol and low gonadotropin levels favor central hypothyroidism (Umpierrez, 2002).
- Newborn screening for hypothyroidism: Congenital hypothyroidism occurs in approximately 1:4000 births and, if untreated, causes irreversible mental retardation, physical deformities, and even death. Screening with T4 and/or TSH levels is advised within 2-4 days of birth, and is performed by various immunoassay methods on blood collected on special filter paper (AAP, 2006)
Alias
- Third generation TSH
- Thyroid stimulating hormone (TSH)
Test Setup Days
Monday through Friday PM shift
CPT
84443 Limited Coverage Test For Medicare.
Advance Beneficiary Notice Of Non-Coverage (ABN) Required
If Diagnosis Is Not Covered.
Frequency Limit Test For Medicare.
Advance Beneficiary Notice Of Non-Coverage (ABN) Always
Required For Frequency.
LOINC: 11579-0
CPT
AGE 0-5 DAYS: 0.700-15.200 UIU/ML
6 DAYS-2 MONTHS: 0.700-11.000 UIU/ML
3-11 MONTHS: 0.700-8.400 UIU/ML
1-5 YEARS: 0.700-6.000 UIU/ML
6-10 YEARS: 0.600-4.800 UIU/ML
11-17 YEARS: 0.500-4.300 UIU/ML
>=18 YEARS: 0.400-4.100 UIU/ML
| UNIT CODE | UNIT CODE NAME | ANALYTE | GENDER | AGE | REFERENCE RANGE | UNITS OF MEASURE |
| 2835 | TSH | TSH | NOT SPECIFIED | 0Y | 0.400-4.100 | UIU/ML |
| 2835 | TSH | TSH | NOT SPECIFIED | 5D | 0.700-15.200 | UIU/ML |
| 2835 | TSH | TSH | NOT SPECIFIED | 2M | 0.700-11.000 | UIU/ML |
| 2835 | TSH | TSH | NOT SPECIFIED | 11M | 0.700-8.400 | UIU/ML |
| 2835 | TSH | TSH | NOT SPECIFIED | 5Y | 0.700-6.000 | UIU/ML |
| 2835 | TSH | TSH | NOT SPECIFIED | 10Y | 0.600-4.800 | UIU/ML |
| 2835 | TSH | TSH | NOT SPECIFIED | 17Y | 0.500-4.300 | UIU/ML |
| 2835 | TSH | TSH | NOT SPECIFIED | 150Y | 0.400-4.100 | UIU/ML |
| 2835 | TSH | TSH | MALE | 0Y | 0.400-4.100 | UIU/ML |
| 2835 | TSH | TSH | MALE | 5D | 0.700-15.200 | UIU/ML |
| 2835 | TSH | TSH | MALE | 2M | 0.700-11.000 | UIU/ML |
| 2835 | TSH | TSH | MALE | 11M | 0.700-8.400 | UIU/ML |
| 2835 | TSH | TSH | MALE | 5Y | 0.700-6.000 | UIU/ML |
| 2835 | TSH | TSH | MALE | 10Y | 0.600-4.800 | UIU/ML |
| 2835 | TSH | TSH | MALE | 17Y | 0.500-4.300 | UIU/ML |
| 2835 | TSH | TSH | MALE | 150Y | 0.400-4.100 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 0Y | 0.400-4.100 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 5D | 0.700-15.200 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 2M | 0.700-11.000 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 11M | 0.700-8.400 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 5Y | 0.700-6.000 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 10Y | 0.600-4.800 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 17Y | 0.500-4.300 | UIU/ML |
| 2835 | TSH | TSH | FEMALE | 150Y | 0.400-4.100 | UIU/ML |